{kind=link}


Story at-a-glance
- A common problem in medicine is that tests and interventions are chosen that do not make sense once the full picture of their implementation is considered. Unfortunately, doctors are not trained to think two steps ahead, and we witnessed this throughout the disastrous COVID-19 response
- Most of the options we ultimately chose to combat the pandemic were ineffective, frequently illegal, at odds with the existing medical evidence and often extremely detrimental to society. Nonetheless, anyone who provided reasonable criticisms to those approaches or suggested effective solutions to stop the pandemic was widely criticized and silenced
- Much of that debacle resulted from three incompetent and dishonest doctors, with the support of the national media, hijacking the COVID-19 response and becoming public health dictators
- Now that plans are being laid to revive the COVID-19 response, it is critical we reflect on the systemic mistakes that were made so we do not repeat those mistakes again
Two of the themes I’ve repeatedly tried to illustrate in my writings are the widespread lack of critical thinking in medicine and the pervasive propaganda apparatus that in many ways has taken its place. I believe both of these are particularly relevant to the current attempts to revive the COVID response.
For example, when someone (thanks to effective propaganda) has a monopoly over the truth, it shields their actions from scrutiny because no one will be able to question if what’s being done makes any sense. Since many of the COVID mitigation policies made no sense, those who became aware of their nonsensical nature in turn refused to follow them, but since many others were shielded from that information, they happily complied with everything.
In this article, I would like to examine some of the major deficits in critical thinking I observed throughout the COVID response in the hope we can avoid making those mistakes again.
Foundational Epidemiology
When COVID first started, there were a variety of unknowns about the virus. One of the most important ones was if it had a droplet or aerosol spread. Some viruses, like influenza (the flu) spread through being attached to water droplets, and for those viruses, “targeting” water droplet spread to varying degrees mitigates their transmission.
For example, while viruses are infinitely smaller than the gaps in a cloth mask, water droplets are not, so if someone wears a cloth mask, the cloth fiber will inhibit the expulsion of water droplets from the mask wearer, and by extension the degree to which they spread influenza. Likewise, the distance water droplets can travel is limited to around 6 feet, as the droplets quickly fall to the ground, so maintaining distance between people reduces the spread of those viruses.
Finally, droplet with viruses will attach to surfaces, after which point, they can be picked up by someone physically touching the surface.
Conversely, if a virus is aerosolized (meaning it freely floats in and travels through the air), none of the above applies. Instead it will spread everywhere, hang around in the air long after someone has left, and penetrates most of the barriers designed to block it.
Aerosolized pathogens are thus known to be much more contagious and the hospitals have much stricter isolation protocols to prevent their spread within the hospital (tuberculosis and measles are the two classic pathogens known for this).
As it so happened, from the start of the pandemic, there was very strong evidence COVID-19 spread through aerosols — for example at the end of January 2020, the Diamond Princess cruise ship experienced one of the earliest COVID outbreaks and was quarantined. The outbreak on the ship was closely studied by experts around the world as it had inadvertently provided the perfect experimental conditions to study how COVID-19 was transmitted.
One of the many observations made was that people who remained in their rooms caught COVID-19, which suggested the virus was spreading through the ventilation system and was thus aerosolized.
Subsequently, numerous other observations also emerged suggesting aerosolized transmission, such as outbreaks occurring where individual indoors were 18 times more likely to catch the virus indoors than those outdoors along with numerous cases of individuals catching COVID-19 from people they were far over 6 feet away from.
By the time the Diamond Princess outbreak happened, I was relatively certain aerosols were a key route of transmission. Yet, despite numerous parties petitioning the WHO with evidence of aerosol transmission, the WHO insisted that only droplet transmission was occurring, and sent out numerous statements dismissing the aerosol hypothesis. Eventually, two years later, the WHO changed their position and quietly announced that aerosol transmission also was occurring.
This monumental mistake prompted Nature (a premier scientific journal) to conduct an investigation to determine exactly how this happened and confirmed that the WHO had ignored an overwhelming volume of evidence for aerosol transmission during that period.
Note: For those of you who cannot view the full article, a summary by Mercola can be viewed here.
This is very similar to many of the other profound lapses of judgement we saw throughout COVID-19 (we will cover throughout this article) where longstanding scientific principles and clear scientific evidence were thrown out the window so a COVID-19 response at odds with the actual science could be conducted.
In short, had aerosol transmission have been recognized, there would have been no justification for either masking or social distancing.
Note: In a 3/21/21 editorial by Scott Gottlieb (one of Trump’s FDA commissioners) stated that no one knew where the arbitrary 6 foot recommendation came from and Gottlieb’s best guess was that it originated from the mistaken assumption that SARS-CoV-2 spread through water droplets.
My best guess is that social distancing originated from a high school sophomore’s 2006 science fair project, and like many things to come in the pandemic industry, was based off of wildly inaccurate computer models.
Critical Thinking and Diagnostic Tests
Within medicine, much of a doctor’s education has shifted to being trained to follow clinical algorithms, standardized protocols, and authoritative guidelines (all of which often but not always improve patient outcomes) rather than doctors using their critical thinking to independently decide what the best approach is for each patient they see.
As the previous example illustrates, being told to have everyone wear cloth masks and socially distance should have raised some red flags, but rather than ask if the recommendations made sense, the majority of doctors instead simply pushed the guidelines they were given onto their patients and community.
One longstanding area that highlights the issues with robotically following protocols is the way diagnostic testing is utilized. When doctors aren’t sure what to do, they typically order standard diagnostic tests to help their guide their approach. While this seems reasonable, the problem is that they often don’t think two steps ahead and ask any of the following before ordering the test:
- Will the possible results of this test in any way change how I treat this patient?
- How likely is this test to harm the patient and does that potential harm outweigh the benefits of the test?
- How likely is this test to tell me something I don’t already know?
- Could an appropriate physical examination tell me what I am trying to figure out with this test?
Note: The last point is a huge issue in medicine, as medical training has gradually shifted away from performing a detailed physical examination (which is often the most useful way to evaluate someone) to ordering lots of expensive tests, which has led to much of the physical examination becoming a lost art in the richer nations. I can’t prove this, but I have always thought this shift occurred to help make money for the medical industry.
Because of all of this, I continually see patients who receive lots of unnecessary tests. For instance, any time a patient is sent to a specialist, the specialist will typically order the bread and butter tests of their specialty even if there is no good justification for doing so.
In many cases, I’ve referred a patient to an appropriate specialist, told the specialist on the phone what I think the patient needs done, why I would caution against using their standard tests for the patient’s specific circumstances, tell the same to my patient, and then inevitably find out that the specialist successfully pushed them to do the test, and in many cases didn’t do anything else.
Eventually, I realized the most effective way to prevent this happening to my patients was to tell them:
The doctor I’m sending you to may want to order this test. If they do, ask them to tell you what possible results could come up from the test, roughly how likely each one is, and how each result would change their management of your case. You can also ask them if there are any potential risks from the test and how much the test will cost, but try to focus on if there is any point to the test in the first place.
The area where I most commonly encounter this issue is with MRIs, which neurologists typically default to using, particularly if they can’t make sense of what’s happening. Whenever an MRI (or CT) is done, you have the option of injecting a contrast agent which makes it easier to see all the details present. With MRIs, the primary contras agent utilized is gadolinium, a metal that due to its magnetic properties, becomes illuminated on MRIs.
Gadolinium is a toxic heavy metal that has the unfortunate side effect of sometimes causing severe permanent illnesses (e.g., neurological disabilities) in those who receive contrast agents containing it. For example, Maddie DeGaray was a child enrolled in Pfizer’s small trial that tested their vaccine in children.
She had a bad reaction which the investigators tried to cover up (as her injury alone would have made the vaccine too dangerous to approve for children), eventually got a gadolinium MRI, at which point she immediately and permanently lost the ability to walk.
In short, because of how many people I’ve run into that developed gadolinium illnesses, I try to avoid those MRIs if at all possible (especially for sensitive patients). In doing so, I have learned that in the majority of cases where neurologists insist on a gadolinium MRI, there is no real net benefit compared to performing a normal MRI (e.g., the final test result will still be ambiguous, or nothing can do done for the most likely diagnosis the gadolinium MRI will detect).
Despite this, and the fact that enough evidence of gadolinium harm has accumulated that many large groups now recommend against it unless absolutely necessary, almost all doctors I meet still push these MRIs.
Note: Manganese is a much safer metal which also has the magnetic properties necessary to functions as a contrast agent. Despite decades of research and data showing it is both safe and effective, it is still not available to patients.
To provide an example that puts all of this into context, many COVID-19 vaccine injured patients I know have seen dozens of doctors (including specialists at premier institutions).
Those doctors have ordered countless (not necessarily safe) tests which cost insane amounts (e.g., one of my patients has seen over 30 specialists, had received almost 100 tests — many which required nuclear isotopes being injection, and their insurance has now paid well over $300,000.00 for those tests), but all failed to detect anything that could be diagnosed (frequently leading to the patient’s being referred to psychiatry).
In many cases, I’ve found this issue emerged because the conditions the vaccine injured have are things the standard tests and labs are simply not designed to detect.
For example, when microclotting occurs throughout the body due to strong positive charges (like those found on the spike protein) shifting the zeta potential to one which causes red blood cells to clump together (explained here), a myriad of different complex issues emerge throughout the body, many of which are due to nerves not getting the blood they need to function.
Those microclots are too small for MRIs to detect, so all MRI’s are “normal.” However in these same patients, when I’ve looked for the microclotting with tests designed to detect it (e.g., by examining the blood vessels of the eyes with a stereomicroscopes) the systemic microclotting can be easily seen.
One of largest failures in critical thinking I observed during COVID-19 came from the infamous PCR tests — the mass adoption of which was justified by the unscientific (and largely proven to be false) assumption that SARS-CoV-2 spread from asymptomatic individuals. These tests had two major issues:
• First their sensitivity was incorrectly calibrated, as the number of times PCR tests amplified existing viral RNA fragments was much higher than appropriate, so the PCR tests would frequently detect SARS-CoV-2 when it was not actually present.
• Secondly (due to the previous point), positive COVID tests often had no correlation with disease outbreaks in communities or the likelihood someone would later become ill. Rather, the only correlation ever observed was the number of COVID cases being directly proportional to the number of tests performed.
The great shame about this was that there was already a reliable and non-invasive way to detect if COVID-19 was going to spike in a community — by testing if it was in the sewage (as COVID lives in your GI tract), and if the amount of it in a community’s wastewater began increasing. However since that was not as alarming as listing thousands of new cases each day, this much more practical approach was never the focus of the pandemic response.
Later, antigen tests were introduced which were much more useful because they could be done immediately (rather than you having to wait to get a PCR result from a lab) and more importantly, did not constantly get false positives.
To illustrate the ridiculousness of all of this, at my hospital, when a patient came in my colleagues did not think needed to be hospitalized, they gave the patient an antigen test (which typically came up negative — and thus did not require them to hospitalize the patient), whereas when a patient came in they felt needed to be admitted, that patient always received a PCR test that invariably came up positive.
Note: A few people I know believe they either got COVID from a nasal swab or suffered a significant injury to their nose as the result of a quick forceful swab at a testing site (which definitely has happened). In many of the cases I came across where the individual caught COVID after a swab, the timeline of events strongly argued for the two being connected.
However, I know Ryan Cole tested numerous swabs and was never able to find SARS-CoV-2 on one Because of this, I think those infections most likely resulted from individuals who were not ill being in close proximity to those who were when they went to get tested and an aerosolized SARS-CoV-2 then infecting everyone there.
Masking
When COVID-19 started in late 2019, I became very worried about it and concluded that I needed to find an effective way to treat it as soon as possible. At the same time, I also recognized that if the HIV response was anything to go off of, it was unlikely an effective treatment would ever see the light of day, especially given that Fauci (who was directly responsible for this happening with HIV) was still in charge — and as you all know, this is exactly what ended up happening.
My thought process in turn was that given the danger the virus posed (based on what I’d seen in China and Italy), I could not risk getting COVID until I felt confident I could treat it. For this reason, I fully admit I was one of the first people in the United States to mask with a fitted N-95 (specifically doing so at work, conferences and when traveling in airports), something many of my colleagues actively made fun of me for doing.
Note: For pathogens with an aerosol spread, N-95’s don’t really work unless they are fitted to the wearer as otherwise they just get in from the gaps between the mask and your face.
Additionally, for many infectious illnesses, the route of infection is often through the eyes or ears, something people rarely consider protecting (e.g., by not touching them), and frequently clearing out the ears (e.g., with hydrogen peroxide) can make a huge difference if done early in the course of a viral upper respiratory illness.
By May of 2020, I felt confident that I could treat COVID-19 and stopped masking entirely except when I was around a patient with COVID or legally required to — at which point those same colleagues were hostile towards me for not (cloth) masking in public.
In short, masking was not something I at all wanted to do, but I felt given all the unknowns at the start, it made sense to mask while I was figuring out how to treat COVID-19. In contrast, most of my colleagues did the exact opposite and did not listen to any of my warnings (which for example resulted in me needing to supply them with PPE I’d stocked up before it ran out).
I believe the difference in our thought processes came about because I always thought two steps ahead, whereas in each case, like I highlighted in the previous section with diagnostic testing, they did not and instead simply did whatever the current guidelines were.
This was particularly frustrating because after my warnings about COVID and then the need to acquire PPE were ignored, no one was interested in the treatments I put forward for treating COVID-19 (as they were not in the guidelines) even when the protocols I found had saved patients otherwise expected to die.
Once the masking kicked into gear, there were a few major points that argued against their mass adoption:
• No one knew how to wear them (it baffles me but I still see medical students who elect to wear masks — when many are not — but don’t even have the mask cover their nose).
• Since more and more evidence accumulated people with masks were getting infected and that COVID had an aerosolized spread, there was no possible justification for cloth masks.
• People developed a variety of health effects from the masks such as difficulty breathing and increased respiratory tract infections.
One of the most interesting ones I learned of came from a few integrative colleagues who had tested the nasal bacterial and fungal flora of their patients for years (as this commonly is applicable for complex illnesses) and found that after the COVID masking, Klebsiella and Pseudomonas (along with a few weirder species) started being frequently found in their patients.
Fauci and Masks
In a recent article, I put forward the argument that people in power will typically lie if it’s possible for propaganda to convince the public they are telling the truth. Fauci’s duplicity during COVID-19 is an excellent example of this, as it can be proven he lied continually, and the manner in which he lied employed many of the classic propaganda techniques.
Consider this February 5, 2020 email Fauci wrote (which essentially matches what I believed at the time):
“Masks are really for infected people to prevent them from spreading infection to people who are not infected rather than protecting uninfected people from acquiring infection.
The typical mask you buy in the drug store is not really effective in keeping out virus, which is small enough to pass through material. It might, however, provide some slight benefit in keep out gross droplets if someone coughs or sneezes on you.
I do not recommend that you wear a mask, particularly since you are going to a very low risk location.”
However, as we all know, Fauci instead became one of the leading cheerleaders for the masks, even after more and more evidence accumulated showing it made no sense at all. Many other politicians followed in his footsteps with equally ridiculous demonstrations:
Note: I suspect they did not do this at home.
As time went on, public opinion turned more and more against the masks. Eventually a Cochrane review (the most definitive form of evidence) was published that determined there was no benefit from cloth masking, a small benefit may occur from N-95 masking (depending on how it was assessed, compared to cloth masking, a -10%, 14% or 30% improvement was observed).
It should be noted that this review also included viruses like influenza which have a droplet spread, which means any of the benefits found for COVID-19 were likely smaller than stated. Given all of that, it’s remarkable to see how Fauci still makes non-sensical lies to defends their use — which even CNN is now calling him out on:
Note: What I find particularly frustrating about the useless approaches we used was that in tandem highly effective ones were never utilized. For example, since COVID-19 was known spread by aerosols and much more severely affected people indoors (since the SARS-CoV-2 aerosols floated in place rather than going away), increasing ventilation (e.g., by opening windows) was a simple and highly impactful approach no one ever used.
Likewise, numerous groups were able to show that safe ultraviolet light frequencies could rapidly neutralize the virus and prevent it from infecting individuals where those affordable (and non-disruptive) UV lamps were deployed.
Compulsive Handwashing
The CDC and many other organizations regularly released guidelines advocating for as much hand-washing as possible. The problem with this is that COVID-19 was never shown to spread through hands contacting contaminated surfaces (not unlike how its transmission was erroneously assumed to be through droplets).
A few physicians pointed this out from the get-go, and by early 2021, Nature one of the top scientific journals had admitted there was no point in repeatedly sanitizing surfaces. Likewise, the recent Cochrane review found regular hand washing at best can cause an 11% – 14% reduction in acute respiratory infections.
Nonetheless, compulsive handwashing became a fixture of the pandemic response. Reminders to wash your hands were everywhere. Individuals were regularly chastised or reprimanded for failing to continually wash their hands for 20 seconds, and before long every surface was being regularly disinfected with toxic chemicals.
As I watched all of this, I could not help but recall that a common feature of obsessive-compulsive disorder is a tendency to compulsively wash one’s hands (sometimes to the point the skin is damaged).
Since individuals with similar neurotic conditions became one of the demographics most committed to the pandemic response, I have often wondered if the mass hand-washing campaign was partly chosen to recruit neurotic members of society to fight for the pandemic policies.
This in turn touches upon a broader point. As I am trying to show in this article, virtually every approach we used to address COVID in 2020 was a hassle for everyone involved and known to have no real benefit in preventing COVID. This argues that the primary purpose of the campaigns was not to reduce deaths, but rather to have each member of the populace do the work necessary to comply with those approaches.
I would argue this actually makes a lot of sense because it is well known in psychology that the more work someone engages in relating to an idea, the more invested they become in supporting the idea.
This principle in turn has been repeatedly exploited by groups seeking to control others all throughout history, including within the United States (e.g., children going door to door collecting scrap metal to be turned into munitions to fight the Nazis — even though the metal was ultimately never used).
Lockdowns
Prior to the vaccines, without question, the most damaging COVID policy were the lockdowns — something I believe was made possible by having the public already be habituated to all of this due to the continual hand washing, social isolation and mask wearing they had already done.
Since those rituals were not sufficient to overcome much of the public’s resistant to these measures, we watched other sneaky tactics be used such as moving the goal posts. For instance, do you remember how long the “Two weeks to slow the spread” ended up lasting for?
Once you got past all the propaganda, the lockdowns made no sense. For example let’s consider what the WHO had to say about all of this in 2019:
“The evidence base on the effectiveness of NPIs (non-pharmaceutical interventions) in community settings is limited, and the overall quality of evidence was very low for most interventions.
There have been a number of high-quality randomized controlled trials (RCTs) demonstrating that personal protective measures such as hand hygiene and face masks have, at best, a small effect on influenza transmission. However, there are few RCTs for other NPIs, and much of the evidence base is from observational studies and computer simulations.
School closures can reduce influenza transmission but would need to be carefully timed in order to achieve mitigation objectives. Travel-related measures are unlikely to be successful in most locations … and travel restrictions and travel bans are likely to have prohibitive economic consequences.
The most effective strategy to mitigate the impact of a pandemic is to reduce contacts between infected and uninfected persons, thereby reducing the spread of infection, the peak demand for hospital beds, and the total number of infections, hospitalizations and deaths.
However, social distancing measures (e.g. contact tracing, isolation, quarantine, school and workplace measures and closures, and avoiding crowding) can be highly disruptive, and the cost of these measures must be weighed against their potential impact.”
Unfortunately, all of this went out the window after a hysteria was whipped up about COVID-19. Shortly before the lockdowns, a model was put forward asserting that a global catastrophe would occur if strict lockdowns were not immediately implemented, and that model was largely responsible for convincing leaders around the world they had no choice but to enact them. To give you an idea of just how “accurate” the model was:
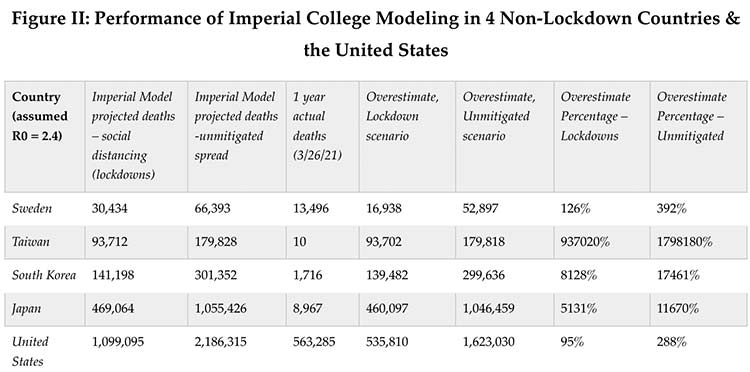
Note: Much of the existing evidence suggests lockdowns increased rather than decreased the COVID-19 death rate.
Many things should have called the Imperial model’s predictions into question (e.g., its author had for decades repeatedly made extreme overestimations of the severity of previous infectious disease outbreaks, and the model itself made no sense).
Yet despite its repeated failures to accurately predict COVID-19, it was never challenged nor updated as data became available showing its core assumptions were wrong. Instead leaders (with a few exceptions like Ron DeSantis) didn’t think the argument through and simply took the most trustable experts at their word.
This was a shame because it should have been obvious the lockdowns (which lacked evidence to support their use) didn’t make even sense once you thought more than one step ahead. Consider each of the following:
- Lockdowns are extremely costly to society, so they cannot be maintained indefinitely.
- Once lockdowns are broken, all the cases that would have been prevented will occur anyways. So at best, they can only delay the inevitable.
- The only way lockdowns can make sense is if they are done within a strategic context such as buying time for an emergency therapy or to ensure individuals are exposed at a later time when they will be the most likely to survive an infection.
Instead, once the lockdowns were pushed forward, every strategically valid follow-up was disparaged. For example:
- Each (non-patentable) COVID-19 therapy that independent researchers discovered was blacklisted — even simple things like encouraging people to take vitamin D or throat and nasal washes (which I now believe, provided xylitol and a disinfectant are used, was the most accessible and effective way to treat early COVID-19 due to the virus initially entering through those routes before it got to the lungs).
- People were encouraged to stay indoors and socially distance over the summer (which for numerous reasons predictably set them up for a bad COVID season right before the election and throughout the following winter).
- The proposal to have those at the lowest risk from COVID go back to their normal lives and develop a natural immunity that could then protect the most vulnerable members of society (both due to their natural immunity slowing the spread and because COVID would, following the laws of virology, mutate to less dangerous strains) was relentlessly attacked — for example FOIA’d emails showed that Anthony Fauci and Francis Collins conspired to torpedo that proposal, and shortly after the national media did.
Unfortunately, since the medical profession once again did not think two steps ahead, the inevitable (and later proven) failures of the lockdowns were never considered. Conversely, the costs of the lockdowns were immense. For instance:
|
According to the WHO, in the first year of the pandemic, global prevalence of anxiety and depression increased by a massive 25%. |
|
Domestic abuse rose by 8.1% during the lockdowns. |
|
There was a general worsening of health. For example to quantify the lockdown’s effects on metabolic health, one study found people gained an average of 2 pounds per month of lockdowns. |
|
Critically important evaluations and treatments (e.g., for cancer) were skipped. Note: There was also an unprecedented drop in sudden infant deaths during the lockdowns, something many people in the vaccine safety community accurately predicted would occur as a result of infants skipping their routine vaccination appointments during the lockdowns. |
|
School closures (which were completely unjustified as children had no risk for COVID-19) had devastating effects on the educational development of students across America — particularly for the poorest children. For example, researchers who had monitored children for years identified a drop from 100 to 78 in the average IQ of children born during the pandemic (which was most likely due to their social isolation and facial expressions being concealed by masking). To quantify the impact of a 22-point drop:
|
|
The lockdowns caused a “historically unprecedented increase in global poverty” of close to 100 million people, and a 11.6% global increase of extreme poverty. |
|
150 million people no longer had the food they needed. The magnitude of this wave of global starvation in another thing that is almost impossible to put into words. |
|
One third of American’s small businesses closed. These were often sources of generational wealth and more importantly, a way to escape from poverty. |
|
We witnessed the largest transfer of wealth in history. From 2020 to 2021, billionaires went from owning slightly over 2% of the global household wealth to 3.5% of it. |
All of the points I made above were entirely predictable, and many of them were explicitly warned against as reasons for not enacting the lockdowns. I would argue that a really good reason would be needed to justify inflicting a single one of these points upon society — yet instead we did all of them (and more) for the lockdowns, which were a speculative measure that ultimately had no benefit.
Had I not subsequently witnessed the COVID vaccine campaign, I would have argued the COVID lockdowns were in contention for the biggest public health mistake in history.
COVID Vaccines
In my opinion, the best argument for the lockdowns was that if they could have been instituted prior to COVID-19 entering a community, that in theory could have permanently prevented a lot of people from getting the infection (although as the WHO’s 2019 report stated, it was unclear if even this was a good idea).
A similar issue existed with vaccinating for COVID-19. If it was somehow possible to vaccinate the entire community for COVID prior to it entering the population and there were relatively few people the vaccines failed for (e.g., the immune suppressed individuals), it might have been possible to make COVID disappear.
However, if that did not happen and only some people were vaccinated once the virus was already there, the virus would simply infect those not immune to it, and then within those infected patients, rapidly mutate to strains not covered by the vaccine and then infect the vaccinated.
Since the vaccines were not available until a year into the pandemic it was essentially a forgone conclusion that all they could do was trigger the evolution of variants the vaccines would not be effective against. Furthermore, from an efficacy perspective, there were three major problems with the vaccines.
First, coronaviruses, and particularly SARS-CoV-2, are known for rapidly mutating. Because of how rapidly they mutate, it had long been considered an immensely challenging task to make a vaccine against them.
Second, the vaccine design chosen only made one antigen (the toxic spike protein). Since this was one of the most rapidly mutating part of the virus, it was a forgone conclusion that the vaccine would rapidly stop working on the currently circulating strains of COVID. Ryan Cole has aptly summarized this as “why are we mandating a vaccine for an extinct virus?”
Third, the immunity the injected vaccine created only existed in the blood (something which the virus enters much later in the infection), meaning that it did not protected against infection and thus transmission — a problem well-known for vaccines that do not create mucosal immunity.
Third, because of how fast SARS-CoV-2 mutates, it is almost impossible to identify an existing strain, produce a matching vaccine to it, and then get it to the population before that variant is already on the way to extinction.
When you consider that the vaccine was also highly experimental and had a huge number of known potential risks, like the lockdowns (provided one thought two steps ahead), it was very difficult to provide a justifiable argument for why it could possibly be a good idea to inject the entire world with this technology — especially if doing so required unparalleled ethical violations.
As it so happens, not only were the vaccines a mistake from the start, we essentially saw the worst case scenario happen with them:
• Every single potential risk turned out to be true, and the spike protein vaccines ended up being one of the most dangerous medical products in history.
• Rather than decreasing COVID-19, in many cases they increased its duration and prevalence (something which has only gotten worse as time has gone forward).
• COVID had originally been projected to have a few waves and then go extinct. After the vaccines came out, this did not happen and instead COVID has now become a fixture in our daily lives that will “require” annual vaccinations like the flu.
While I can’t prove this, I long thought the reason why there was such a desperate push to rapidly get a vaccine for COVID to the market was so that a vaccine could be created for the virus prior to it becoming extinct and the market no longer existing.
Consider for instance that numerous countries in Africa never instituted the COVID-19 vaccines, and COVID long ago disappeared from those countries.
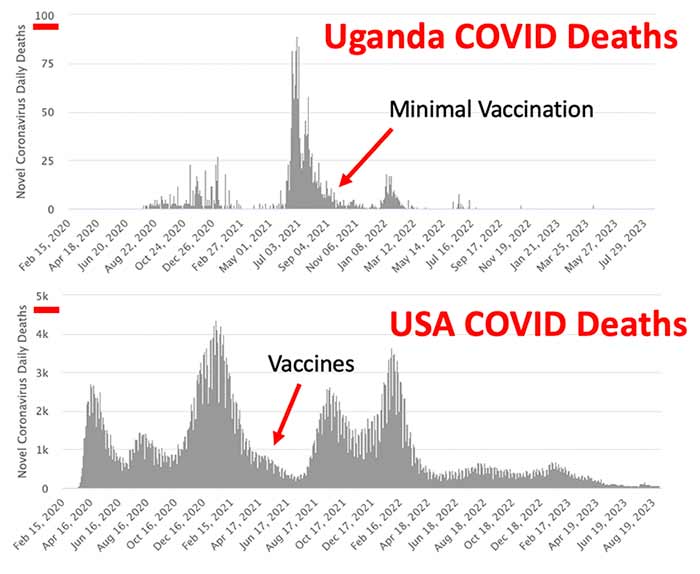
Note: Uganda has less people than America, while the total number of deaths is much larger on the USA graph. To illustrate the deaths proportional to the population, the USA graph should have been about 7 times larger than it was.
Because of how rapidly SARS-CoV-2 mutated, many of us believed from the start that the only way to address it was by allowing people to get the infections, provide treatments to mitigate the danger of their infections and then allow them to develop natural immunity (which is much harder for the virus to evolve resistance to). As we all know, this was not what happened.
Instead, we are now seeing the toxic vaccine become normalized as an annual required product. Sadder still, the goal posts have moved to the point not only our top public officials, but even a Pfizer executive (the previously mentioned former FDA commissioner Scott Gottlieb) is promoting it on national television.
Who Was Responsible for the Pandemic Policies?
Joe Navarro and Scott Atlas M.D., in each of their White House memoirs provided the best summaries I have come across of what went awry during the COVID-19 response.
Joe Navarro
Navarro recognized early on that COVID-19 would turn into a huge problem, but when he tried to initiate something being done, the rest of the administration shut him down because they didn’t agree with his dire forecasts. Eventually, Navarro was able to convince Trump to go against the experts (e.g., Fauci) and initiate a travel ban from China (which was widely decried in the media).
Later, once the pandemic started, he observed that the pandemic response was dysfunctional and kept on (unsuccessfully) trying to push for viable treatments like hydroxychloroquine (HCQ) to be used to treat the virus. The roadblocks he ran into were quite illuminating:
“On March 23, four days after President Trump had promised that the FDA would expedite the use of HCQ, [HHS Secretary] Azar and his deputy at HHS, Bob Kadlec, gave several FDA bureaucrats very clear and explicit instructions to make hydroxychloroquine widely available to the American public as an early CCP Virus treatment on an outpatient basis.
Nonetheless, five days later, those very same FDA bureaucrats — including FDA commissioner Stephen Hahn and his eventual replacement, Janet Woodcock — completely countermanded the POTUS-Azar-Kadlec order. Instead, on March 28, the FDA issued a rogue directive restricting the use of HCQ to the late treatment of hospitalized patients.
With its rogue directive, the FDA effectively ensured that HCQ would be diverted from its best possible use as an early treatment for outpatients [where it worked and save lives] to its worst possible use as a late-treatment medicine for hospitalized patients. At least in the court of public opinion, that single decision was tantamount if not to murder, then certainly to negligent homicide.
Yet there would be even more blood on Anthony Fauci’s hands … when it was Fauci’s turn [at the COVID task force], right on cue, he immediately played his “there’s only anecdotal evidence card. Just as immediately, I stood up from my backbench chair just behind Vice President Pence and walked straight toward Fauci.”
As I approached him, I saw fear in his eyes. I’m sure it crossed his mind that I might physically assault him. Instead, I dumped my large dossier of studies onto the table in front of him and said to Fauci as much as to everyone else in the room — especially VPOTUS — “Tony, these are not anecdotes. That’s more than fifty scientific studies in support of HCQ.
Fifty! So stop spouting your crap about there only being anecdotal evidence because not only is it counterfactual. You are going to kill people just like you did during the AIDS crisis when you refused to approve medicines that everybody but you knew worked.”
As if all that weren’t bad enough, on April 23, FDA commissioner Stephen Hahn took yet another rogue and inexplicable action that would blow even more fetid air into Hydroxy Hysteria’s billowing sails.
Under Hahn’s signature, the FDA issued a “Drug Safety Communication” that warned of “abnormal heart rhythms and possible death” associated with HCQ [which was due to one study that deliberately gave toxic doses to patients]. The FDA also warned practicing physicians that the drug should be used only in hospital settings and not with outpatients.
The ludicrous new “Fauci-Hahn-Woodcock National Pandemic Strategy” would keep early-stage infected patients quarantined at home and without hydroxychloroquine treatment until they became so ill that they had to be admitted to a hospital.
Once in hospital, they would finally be given hydroxychloroquine, which, in that late-treatment use, would not work very well. It can’t be said too forcefully: what the FDA did was flat-out Grim Reaper ridiculous.”
As a result of the FDA’s warning, demand dried up for HCQ, doctors became scared to prescribe it, facilities stopped allowing it to be prescribed, and it became impossible for doctors to recruit patients for further HCQ trials. Navarro found this particularly frustrating as he had had the foresight to stockpile enough HCQ to treat COVID-19 throughout America, but instead no treatment for COVID was ever made available and hundreds of thousands of Americans died.
However, no bad deed goes unrewarded, and roughly a year later, Commissioner Hahn, left his position and became the Chief Medical Officer for Moderna’s parent company.
Not long after in June, despite highly questionable evidence of safety or efficacy, Azar signed a deal to buy the entire supply of remdesivir (approximately 500,000 doses) for roughly 3200.00 per treatment course. It was estimated the fair price for each course of treatment was around 310.00 (while the production cost was approximately 10.00).
Typically, when the government makes an investment of this scale (e.g., both in the development and acquisition of remdesivir), it will always do everything it can to utilize the investment regardless of how dangerous and ineffective the product turns out to be (this likewise is one reason there has been such a push to “use” all the vaccines the government already paid for).
Almost everything Navarro described in the HCQ saga was identical to what my colleague and friend Pierre Kory experienced with the agencies conspiring to block Ivermectin from being used to treat COVID, so I can deeply empathize with how frustrating all of this must have been for Navarro.
Scott Atlas M.D.
Once the lockdowns began, Atlas (a highly regarded academic physician) became an outspoken critic of the lockdowns as he realized they had no benefit and were causing massive harms to the country. Trump eventually reached out to him and asked him to join the White House’s COVID task force as he felt Atlas’s approach was correct for America.
Once there, Atlas realized that everyone in the White House was deferring to the expertise of the three doctors on the COVID-19 task force, and that Anthony Fauci, Deborah Birx, and Robert Redfield (the CDC director) were effectively directing the entire COVID response. Later it was discovered they shared a questionable past together and all three had made a pact to quit if Trump dismissed any one of them from the task force.
For example, in the early 1990s, Redfield and Birx, both army medical officers, worked together on a HIV vaccine and published fraudulent data suggesting it worked. They were investigated by the military and charged with deliberate scientific misconduct and fraud which Redfield confessed to.
Nonetheless, Redfield then lied to congress, claiming his vaccine worked (it didn’t) and was able to secure a 20 million dollar grant to the military for his vaccine, which in turn led to all the charges being dropped and kickstarted Redfield and Birx’s advancement through the Federal bureaucracy.
Note: Fauci was also heavily involved in the HIV vaccine research, but like his colleagues never found an effective vaccine.
During his time on the task force, Atlas was struck by the gross incompetence he witnessed, particularly in Fauci and Birx, as they frequently demonstrated an inability to grasp simple concepts in scientific publications to such a severe degree Atlas was doubtful either of them could have completed a medical residency now.
Many of the examples he observed were almost surreal and he came to refer to the COVID task force as the Mad Hatter’s Tea Party (I personally felt Atlas’s account most closely matched the presidential cabinet meeting in Idiocracy).
The central issue with the task force was that from the start Birx became convinced the only solution for the pandemic was to conduct as much testing as possible and then use the positive cases those tests yielded to justify mask mandates and scaring governors into locking down their states (leading to many Republican governors to complain to Atlas about the useless advice Birx was continually giving them).
Regardless of the arguments or data Atlas raised (e.g., that COVID was not dangerous to children so there was no reason to lockdown schools), he could not get Birx to change her mind, and in the cases where he gained any type of momentum against her policies, she would demonstrate remarkable demonstrations of emotional immaturity.
In the rare cases where Atlas was able to make progress with convincing the rest of the task force to move away from endorsing lockdowns, and instead towards targeted protection of the most vulnerable groups (particularly the elderly), someone would leak what happened on the task force to the national media.
A hysteria would then immediately flood the airwaves (often bolstered by statements Fauci gave to the press) alleging the herd immunity strategy sacrificed large numbers of American lives for the economy, which in turn led to Atlas’s proposals being rolled back to avoid the political backlash the strategy they would cause prior to the election.
A quotation from a review of Atlas’s memoir perfectly summarizes much of the what happened within the White House during the pandemic response:
“When he resigned from the Task Force in a telephone call to Trump, Atlas writes, the president told him, “You were right about everything, all along the way. And you know what? You were also right about something else. Fauci wasn’t the biggest problem of all of them. It really wasn’t him.”
Trump meant that it was Birx, and Atlas couldn’t resist a parting shot at the aides who had been so afraid of her. Knowing that they were listening on the speakerphone in the Oval Office, Atlas said, “Well, Mr. President, I will say this. You have balls. I have balls. But the closest people around you — they didn’t. They had no balls. They let you down.” They let down the rest of the country, too.”
Note: One of the most telling examples of Birx’s conduct occurred in July 2022 after she left the COVID task force (she ironically is the chief medical officer for a private company that uses UV light to disinfect an area from things like COVID-19). In the July 2022 interview, she admits they overplayed the vaccines and that she knew they would not protect against infection:
Conclusion
I believe you can argue many of the immense errors we witnessed during the COVID-19 response occurred due to it being entirely unscientific.
For example, the most appropriate way to have scientifically decided how to handle the pandemic would have been for an international team of experts is each relevant field (e.g., economics, epidemiology, virology, immunology, vaccinology, molecular biology, and evolutionary biology) to have been convened and vigorously debated which approach made the most sense.
Instead, because the media covered for them, a small number of doctors who were entirely incompetent within those fields were able to become public health dictators with absolute control over everything that happened. As a result, we all paid the price for their terrible decisions (e.g., their single minded focus on trying to free up hospital beds in the short term by isolating everyone), while many of them (e.g., the two FDA commissioners) got paid off for selling out America.
Consider for a moment how the WHO’s 2019 guidance for handling a respiratory pandemic compared to what was actually enacted throughout 2020 and 2021:
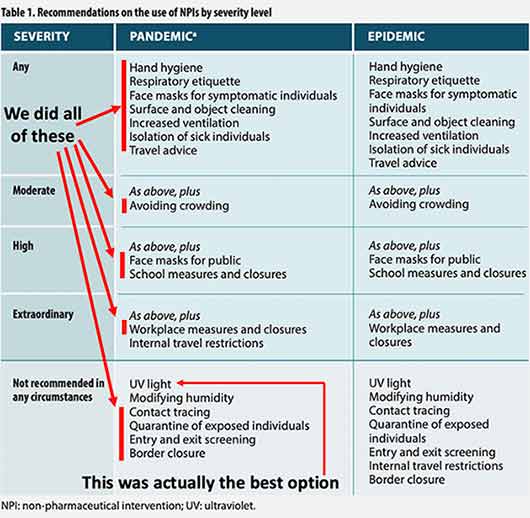
After I began to hear reports over the last month along with more and more signs that many of these measures may be brought back this fall I felt I need to write this article and review the historical context behind what happened.
For instance, because of absurdity of mask mandates, Trump blocked the CDC from implementing one, but less than a month after Biden became president, the CDC instituted a nationwide mandate which affected all airline passengers in the United States.
A few months later, a lawsuit was filed against the Biden Administration alleging that the CDC had exceeded its statutory authority by implementing the mandate, and as many of you might remember (everyone on my plane broke out in applause), on April 18th 2022, a federal judge sided with the plaintiffs and overturned the mask mandate.
The CDC requested for the Department of Justice to overturn this ruling, which caused 23 states concerned about the CDC’s illegal overreach to have their Attorney Generals file an amicus brief in August 2022 opposing the ruling ever being appealed (17 congressmen also did the same). As the illegality of the CDC’s national mask mandate was quite clear, it took a year for Biden’s DOJ to come up a creative way to overcome the initial ruling.
In May 2023, the Biden administration ended the COVID-19 emergency and then moved to have lawsuits filed against their conduct throughout the pandemic be declared moot and dismissed. For masks, the moot point argument won, leading the 11th Circuit Court to eventually rule on 6-22-23 that:
“Here, the government has carried its burden: there is no reasonable basis to expect the Mandate will be reinstated if this case is rendered moot … and there is not a grain of evidence that the CDC has any plans to promulgate an identical mandate.
We find Appellees’ contention that there is a reasonable expectation that the CDC will issue another nationwide mask mandate for all conveyances and transportation hubs to be speculative at best.
Accordingly, the order and judgment of the district court are VACATED, and the district court is instructed to DISMISS the case as MOOT.”
As legal resources are limited, even at the DOJ, I assumed the Biden administration was putting so much work into appealing the judge’s ruling because they wanted to reinstate unpopular national mandates in the future. Given that, it is something to behold that promising there would be no future mask mandates was the tactic ultimately used to remove the barriers to bringing the mask mandates back.
A Note From Dr. Mercola About the Author
A Midwestern Doctor (AMD) is a board-certified physician in the Midwest and a longtime reader of Mercola.com. I appreciate his exceptional insight on a wide range of topics and I’m grateful to share them. I also respect his desire to remain anonymous as he is still on the front lines treating patients. To find more of AMD’s work, be sure to check out The Forgotten Side of Medicine on Substack.
Source: Original Article
Publish Date: 2023-09-23 05:22:55