{kind=link}

Story at-a-glance
- The SSRI antidepressants are some of the most harmful medications on the market, but also some of the most profitable
- Since their discovery, a deluge of data has shown that they are incredibly unsafe, relatively ineffective in treating depression and very difficult to safely withdraw from
- Thus, to get the SSRIs to market, a wide range of dishonest tactics needed to done to conceal those issues
- Those same tactics have been used to push many of the other worst pharmaceuticals onto the market (e.g., the COVID-19 vaccines). In this article, I will attempt to expose these practices
Every now and then, a highly profitable pharmaceutical will come along that everyone also knows is quite dangerous. Remarkably, rather than this stopping the product, it will often be pushed to market and the profits it generates will be used to ensure any objections to its safety get ignored and blown to the wayside.
One of my goals in writing has hence been to review the scandalous history of some of the most dangerous pharmaceuticals on the market. This was done both to help those being harmed by them (e.g., consider the story of the statins and the story of the NSAIDs) and to illustrate that the horrendous malfeasance we’ve observed from the FDA throughout COVID-19 is in fact has been it’s standard operating procedure.
For example, I recently covered the story of Merck’s Vioxx, an unsafe and unneeded painkiller which was kept on the market until outside investigators proved it was causing heart attacks and strokes (estimated to have killed 120,000 people by the time Vioxx was withdrawn), something Merck was fully aware of from the start.
Vioxx resulted in a wave of lawsuits which cost Merck billions of dollars but never resulted in criminal charges against any of the executives responsible for those deaths (rather they got bonuses).
Immediately after the Vioxx lawsuits, Merck brought the HPV vaccine Gardasil to market, fully aware that it had minimal value to those vaccinated (in fact it increased the risk of cancer by 44.6% in those who already had the target HPV-16 or 18 infection — something which like COVID-19 is never tested for prior to vaccination). More importantly, Gardasil had an extraordinarily high rate of adverse reactions.
Note: In its trial, over 50% of the girls were observed to have developed “new medical conditions,” 2.3% of which Merck admitted were autoimmune in nature (although the actual figure was likely much higher).
Once Gardasil hit the market, the CDC and FDA were deluged with a wave of injuries being reported to them. However, rather than listen to these warnings, they doubled down on their claim the vaccine was “safe and effective,” did everything they could to bury those injuries, and ardently worked with Merck to sell the vaccine to as many people as possible.
However, as bad as those stories are, I believe what happened with the Selective Serotonin Reuptake Inhibitor (SSRI) antidepressants is even worse. Since the SSRI saga provides the clearest case study I know of into the gross malfeasance of the FDA, this article will review it in the hope we can better understand the agency’s behavior with the COVID vaccines and just how far it will go to protect the pharmaceutical industry.
Note: Psychiatric medications are one of the most profitable drug franchises, making approximately 40 billion dollars a year — a figure that is expected to significantly increase in the years to come.
The Harms of SSRIs
When integrative physicians are asked to name what they consider to be the five most dangerous mass prescribed drugs in America, SSRIs (and SNRIs) almost always end up on the list, something I believe is due to their mechanism of action (and adverse event profile) having many overlaps with an illegal stimulant like cocaine. In the first and second parts of this series, I attempted to detail those harms which included:
|
Causing violent psychotic behavior which frequently led to suicide, and less frequently to homicide. 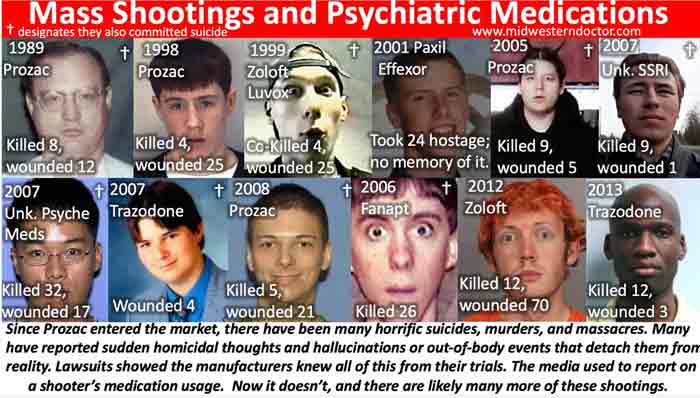
To illustrate: A peer-reviewed Swedish study looked at information on over 850,000 patients prescribed SSRIs within a national database and compared the rates of violent crimes committed by these individuals when they were and were not taking an SSRI over a 3 year period. This study found that SSRIs increased the rate of violent crimes committed by 43% in those between the ages of 15 and 24 receiving the drugs. Note: I initially focused on psychotic SSRI violence because it is a common but undiscussed thread in mass shootings (and other grisly murders which shocked their community). However, I believe the SSRI suicides (as they are far more common) are an even bigger issue. Consider for instance that one study found 10% of mentally healthy volunteers on an SSRI became suicidal, while a much larger survey of SSRI users found 39% had experienced suicidal ideation while on the drugs. Additionally, as the previously mentioned Swedish study shows, SSRIs have been repeatedly shown to significantly increase the incidence of hostile (but not yet psychotic) behavior. |
|
Causing 7.7% of the users each year to develop bipolar disorder (ultimately affecting between 20-40% of SSRI users). For many, bipolar disorder is a permanently debilitating disorder which significantly impacts one’s quality of life. |
|
Causing over half of the users to no longer feel like themselves and in many cases as though they were losing their own minds. |
|
Emotionally anesthetizing 60% of the users. This numbness frequently results in individuals losing the will to leave a toxic relationship or work situation (often for years if not decades), to stop emotionally reacting to things you should react to (e.g., someone being mean to you or violating your boundaries), and to no longer experience the joy or vibrancy of life. |
|
Causing sexual dysfunction in the majority of the users (59% in this study, 62% in this study) which is often extremely impactful to the patient’s life (e.g., 40% in this study found the side effect intolerable). Note: Keep in mind that sexual dysfunction is one of the fastest ways to make someone depressed. |
|
Increasing the risk of life threatening birth defects by 2-6 times (e.g., taking a single SSRI increases the likelihood of the newborn having a septal defects from 0.5% to 0.9%, while taking two increases it to 2.1%). |
|
Causing severe withdrawal symptoms (e.g., frequent electrical zaps through the brain) in 56% of those who discontinue the drugs, with most (46% of discontinuers) experiencing severe withdrawals. Very few people appreciate just how difficult it can be to get off an SSRI (even after only a brief course of the drugs), or that there is absolutely no support within the conventional medical field for patients wishing to get off the drugs. This is particularly tragic because many of the SSRI suicides and murders are preceded by someone having their SSRI dose changed (e.g., increased, decreased or changed to a different medication). Note: Since I was repeatedly asked to do so, I attempted to put together my suggestions on how to withdraw from SSRIs, and I must emphasize it is truly unfair just how addictive these drugs can be. |
Sadly in addition to those common side effects, patients also experience a variety of debilitating side effects from the SSRIs such as palpitations, anxiety, and insomnia. Worse still, it is fairly feasible to identify who will have a good or bad response to SSRIs (e.g., from their genetics) but physicians are never taught how to do this as it would understandably reduce SSRI sales if they were only given to those who will benefit from them.
Note: Similarly much (but not all) of the harm which occurs from vaccines (especially in children) could be avoided if doctors were taught to recognize the initial adverse reactions children experience and pause giving those children additional vaccines.
Likewise, if the vaccines were spaced out (rather than all being given together during the critical developmental period of a child) or the most dangerous ones (e.g., Gardasil or COVID-19) were taken off the market, the harm also would significantly decrease.
However none of that has been done since it would be equivalent to an admission vaccines are not “100% safe and effective” and hence significantly reduce vaccine sales. Consider for instance that the government was actually mandated by the 1986 National Childhood Vaccine Injury Act (which gave legal immunity to the vaccine manufacturers) to study the safety of the existing vaccines so that safer ones could be developed, but it has nonetheless refused to do so ever since.
Regulatory Failure
When you read through the previous section, the first thing that should catch your attention is how just high the percentage of adverse reactions were (e.g., many affected approximately half of those taking the drugs). This in turn highlights just how badly the FDA can fail to do its job and “detect” patently obvious side effects which were seen throughout each SSRI’s clinical trials and then throughout America once the drugs entered the market.
To explain this, I put forth the argument that a drug’s approval is not based on its risks versus its benefits, but rather its risks, its benefits, and its potential profitability (e.g., consider how large the potential antidepressant market is). This for example is why fairly safe and effective treatments (e.g., hydroxychloroquine or ivermectin) were relentlessly attacked as unsafe and ineffective by the American medical establishment.
Similarly, it’s why incredibly dangerous and unsafe ones that were also incredibly profitable were pushed on America throughout the pandemic despite widespread public opposition to their adoption and study after study showing the official pandemic policy was causing more harm than good. Likewise, because people are creatures of habit, you can be relatively assured that if something was used in the past which “worked,” you will see it done again and again.
My familiarity in turn with the dirty deeds by used by the pharmaceutical industry with their worst products (e.g., the SSRIs or Gardasil) in turn made me immediately spot those same tactics being used to doctor the COVID vaccine trials, trick the public into buying them, and cover up the deluge of evidence they were harming people.
As you review the SSRI saga, it is important to remember that much of this was only discovered through lawsuits against the manufacturers and Congressional investigations (as the industry has successfully argued their raw data is proprietary information and hence cannot be disclosed to the public — which in turn requires us to “trust” their presentation of it).
Since that time, the pharmaceutical industry has gained much greater control over both the media and government and has legally been granted almost complete immunity from being sued for an unsafe and ineffective vaccine so similar documents are highly unlikely to be revealed through the discovery process.
Note: In an 1989 lawsuit which followed a man shooting eight people dead, wounding another 12 and killed himself one month after he started fluoxetine, Lilly “won” a jury verdict and claimed it was “proven in a court of law … that Prozac is safe and effective.” The trial judge however forced Lilly to admit that it had made a secret settlement with the plaintiffs during the trial and, outraged, the judge changed the verdict in Lilly’s favor to one of “dismissed as settled with prejudice.”
As part of this deal, Lilly illegally regained the incriminating documents it had been forced to disclose, preventing them from being used in other in other lawsuits. Sadly, in addition to burying incriminating documents within the courts, both the FDA and the EMA (Europe’s FDA) have repeatedly managed to “lose” documents in their possession which incriminated the SSRIs.
Doctoring Trials
While we hold randomized controlled trials in high regard, in truth there are a variety of ways they can be doctored to arrive at the results the sponsor wants, regardless of how ineffective or unsafe they are. For example, the public was told over and over that the COVID vaccines were safe, effective, and would end the pandemic despite:
• The Pfizer trial showing that at best you needed to vaccine 119 people to prevent a single minor case of COVID (e.g., a sore throat plus a positive test), 2711 to prevent a major case of COVID (major being undefined), well over 21,720 to prevent a single death and that the vaccine’s ability to prevent transmission had never been tested.
Note: Once the vaccine hit the market, COVID rapidly evolved resistance to the vaccine, so in real life the actual figures were even worse.
• That many of the Pfizer trial participants experienced symptomatic reactions from the vaccine which were as bad or worse than a COVID infection (e.g., 59% experienced fatigue after Pfizer’s vaccine, whereas around 10-15% experience fatigue after a typical influenza vaccine).
• The Pfizer trial 6 month report showing that more people died (and were injured) who got the drug than who got the placebo.
• Numerous whistleblowers coming forward and testifying they suffered a severe reaction to the COVID-19 vaccine which never made it into the final trial report, one of whom directly notified the senior management at the FDA over what was occurring and another, who (being a lawyer) filed a formal governmental inquiry against the lead author of Pfizer’s vaccine trial.
• A manager of a Pfizer trial site providing documented evidence to the FDA that their site was flagrantly violating established research protocols (e.g., not having the trial be blinded, failing to test those who received the vaccine and developed COVID like symptoms for COVID and underreporting vaccine injuries).
Note: The FDA refusing to listen to reports of serious issues with its drug (and in turn denying they even existed) is likewise nothing new (e.g., I recently provided footage of them doing it the 1980s with the now withdrawn DTwP vaccine). Similar, consider Kim Witczak’s experience:
“As the head of FDA division Dr Bob Temple and Dr Tom Laughren told us in a private meeting with them, David Healy and another family, my husband was just an “anecdote” because it didn’t happen in a double blinded placebo controlled trial [even though lawsuits later showed it did].
I kept telling them to go investigate how my husband went from not sleeping (reason for prescription) to head outside body looking in to hanging in 5 weeks with no depression or history of depression or mental health issues.
It was first glimpse that FDA has no desire to investigate and also learned the same people responsible for approving drugs were also responsible for monitoring safety. Obviously, it is out of control with covid vaccines.”
Given all the serious issues which had been detected in their trial, let’s review how Pfizer described their vaccine in their much heralded December 2020 NEJM paper:
“The safety profile of BNT162b2 was characterized by short-term, mild-to-moderate pain at the injection site, fatigue, and headache. The incidence of serious adverse events was low and was similar in the vaccine and placebo groups.
A two-dose regimen of BNT162b2 conferred 95% protection against Covid-19 in persons 16 years of age or older. Safety over a median of 2 months was similar to that of other viral vaccines.”
At the time this paper was released, it was greeted with an almost religious jubilation by the medical field, and before long I realized it was an exercise in futility to explain to many of my colleagues why the trial’s conclusion was not at all supported by the data within it. As you all know, that jubilation quickly spread through the country and before long gave rise to the highly unethical vaccination mandates.
However, despite a litany of evidence emerging which showed that Pfizer’s paper had serious shortcomings which should not have passed peer review (e.g., documented fraud by the lead author) NEJM has not issued a retraction or correction. This is identical to what NEJM did with its pivotal Gardasil paper, and what NEJM did with its Vioxx paper until a wave a lawsuits mounted against Vioxx (at which point NEJM issued a “statement of concern”).
Sadly, we were warned in 2004 by NEJM’s editor-in-chief that the medical journals (e.g., the NEJM) are corrupt and cannot be trusted. Had she been listened to, there might have been a bit more skepticism towards Pfizer’s NEJM trial.
Note: For those interested, some of the best resources I’ve come across for the tricks drug companies commonly use to create the illusion a bad drug is “safe and effective” are Doctoring Data (by Malcolm Kendrick), Deadly Medicines and Organized Crime (by Peter Gøtzche), The Truth About Drug Companies (by Marcia Angell) and Bad Pharma (Ben Goldacre).
Of these doctors, Goldacre is the most orthodox one, so I find his book on pharmaceutical corruption, while not as good as the previous, is often more effective for persuading more skeptical parties.
The SSRI Trials
The less concrete a pharmaceutical’s benefit is (e.g., preventing minor flu like symptoms occurring in parallel to selectively applied [and almost always positive] COVID-19 PCR tests), the easier it is to alter the trials parameters to create the illusion that a minor change is actually a big deal (e.g., Pfizer’s 0.8% reduction in the likelihood of having a minor case of COVID).
Since “depression” is a highly subjective metric, a variety of methods were concocted to create the illusion the drugs “helped,” improve depression. This for example was done by using scales which “quantified” the effects of the drugs for anxiety and depression rather than something which directly correlated to either.
To illustrate, in a meta-analysis conducted by GSK, suicide-related events occurred more often (3.86 times) on Paxil than on placebo in children and adolescents, whereas suicide items on rating scales the trials used like Hamilton’s didn’t show this difference.
Likewise, a meta-analysis carried out by the FDA in children and adolescents found suicide items on depression scales “showed” SSRIs decreased the risk of suicide by 8% whereas raw company data showed the risk was increased by 95%.
Note: The subjectivity of what constitutes depression has resulted in a significant discrepancy between the benefits psychiatrists perceive from their medications, and what their patients experience. This 1982 study of the effect of blood pressure medications for instance excellently illustrates the tendency of doctors to overestimate the benefits of their drugs:
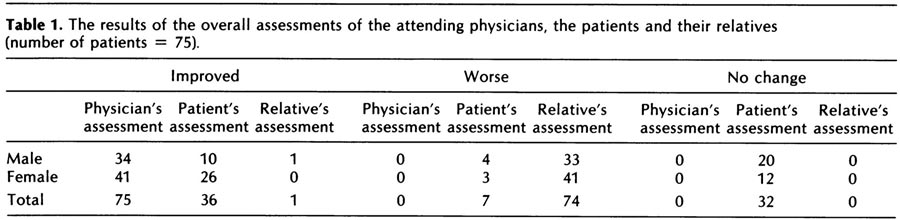
Likewise in the SSRI trials, it has frequently been observed that psychiatrists tend to document a much greater improvement for their patients than what the patients themselves reported.
For example in 8 trials, which included 1576 children and adolescents, trial site psychiatrists reported an overall improvement (effect size 0.25), whereas the patients themselves did not (effect size 0.05), results which were also found in a Cochrane review of newer antidepressants in children and adolescents (effect sizes of 0.29 vs. 0.06).
Given that “mental health” is entirely in the mind of the patient, it is insidious that psychiatrists can be the arbiters of the benefits of these drugs, and we routinely see countless cases where psychiatrists exercise their power to forcefully medicate patients.
Beyond the fact that many of the common SSRI side effects mentioned previously (e.g., sexual dysfunction) would make one “depressed,” in my eyes, one of the best proofs of the absurdity of the SSRIs was that high rate of people who voluntarily stopped taking SSRIs (e.g., between 44%–56% of those in surveys of thousands of patients on SSRIs, and likewise similar results were observed in the clinical trials).
Given that so many patients, against the advice of their doctor were willing to stop using the pills that were supposed to make them feel “good,” this suggests the pills failed to accomplish their goal (i.e., instead it made them feel bad).
Note: Likewise, a survey of 500 patients found 81.5% were unsure if their anti-depressants were necessary.
Conversely, the industry effectively concealed the wide range of side effects which came up in the trials through the following methods:
|
They intentionally harmed the placebo group so that the “drug” group would look better in comparison. This was accomplished by recruiting people into the trials who were already on SSRIs, and then withdrawing those in the placebo from their drugs causing them to enter devastating withdrawals (the side effects of which were detailed in the previous article). Note: Sadly this abhorrent tactic is not unique to the SSRIs. For example, with Gardasil, those in the placebo group were given the most toxic component of the vaccine (its extremely potent aluminum adjuvant), which resulted in similar amounts of severe injuries (e.g., the autoimmune disorders) developing in the “placebo” group, which in turn was used to argue Gardasil’s side effects were unrelated to the vaccine. |
|
They gave the patients who suffered “activating” side effects (e.g., aggression, bipolar disorder, violent behavior, or anxiety) from the drugs benzodiazepines to “treat” those side effects (which of course were not disclosed in the trials since the patients did not display those behaviors when the trial concluded). Note: By one estimate 84% of the SSRI trials used benzodiazepines as part of their protocol. |
|
They used scales to evaluate adverse effects of the drugs which did not register the common side effects of the drugs, which in turn led to many not being detected. Note: This is similar to how Merck chose to label the deluge of Gardasil injuries as “new medical conditions” and how many who participated in the COVID-19 vaccine trials were not given a way to report their injury, even when they repeatedly tried to do so (hence leading to there being “no data” the injury could occur). Likewise, in the system the CDC made to monitor adverse reactions to the COVID-19 vaccine, participants were not given the option to enter many of the more severe COVID-19 vaccine side effects. |
|
They recruited the healthiest members of society (e.g., those less likely to commit suicide) to the trials, and in three-quarters of the SSRI trials they had an initial 1-2 week period where those who had a bad reaction to the drug could be detected and excluded from continuing in the trial. Conversely, many of those who receive SSRIs in real life already have a mental illness, and those who have a bad reaction to the SSRI are almost never withdrawn from it by the prescribing doctor (rather the dose is often raised). Note: This is a longstanding issue in clinical trials (e.g., we rarely test drugs on the elderly — who are typically the most likely to suffer adverse reactions to them, but once the drugs go to the market, those are the groups they are most frequently pushed upon). In the COVID-19 vaccine trials, in addition to relatively few of the elderly being tested (who in turn were frequently found to have the highest rate of death from the COVID-19 vaccines), those with pre-existing autoimmune disorders were also not tested. This was unfortunate because one of the most common severe side effects of the COVID-19 vaccines was an exacerbation of a pre-existing autoimmune disorder (which happens to between 1 in 3 to 1 in 5 of those patients) — something many suspected would be a problem with the vaccine due to its design, but something that conveniently was never assessed prior to it being given to humans. |
|
Individuals were carefully monitored throughout the trials to ensure they do not miss a dose (to avoid a withdrawal) and often taken out of the trial before severe side effects could emerge, something which again does not occur in real life. Likewise, they received an attentive circle of social support (which is very helpful for mental illness but again often does not occur in real life). |
|
They often failed to publicly report severe adverse events (a commonly used excuse is that the investigators decided the events were “unrelated” to the drug). For example, in a pivotal Paxil study, after three subjects were removed from the trial because they attempted suicide, the lead author failed to report this and instead stated that they were terminated from the study because of “non-compliance.” Note: That author also received hundreds of thousands of dollars from the pharmaceutical industry each year which he failed to disclose (along with his department receiving $50 million in “research” funding). Additionally, a social worker found evidence he outright fabricated some of the adolescents who were allegedly enrolled in that trial (as he was paid $25,000 for each child he “recruited”). Despite all of this, he has received no significant repercussions for his actions. Likewise, a 1985 in-house analysis of placebo-controlled trials for Prozac found 12 suicide attempts on Prozac versus one each on a placebo and a tricyclic antidepressant, but after the blind was broken, six of the suicide attempts were “removed” from the dataset. Similarly, the FDA’s expert on safety matters, David Graham, noted that fewer than 10-20% of fatal effects were reported for Prozac, but the data nevertheless showed relatively more suicidality among patients on Prozac than among those on tricyclic antidepressants or placebo. Sadly, all of these warning were ignored by the FDA leadership. Similarly, consider the early 2000s trials where Lilly unsuccessfully tried to promote the use of Cymbalta for urinary incontinence. In these, it was discovered that there had been had 41 deaths and 13 suicides in the trial participants Lilly concealed from the public, including a notorious 2004 case where a healthy 19-year-old student who had joined the trial to help pay her college tuition hanged herself in a laboratory run by Lilly. It was then discovered the FDA had no record of her suicide or that of at least 4 other test subjects and refused to release the data (e.g. deaths it had received) under the logic it would be “commercially unfair” to Lilly if it did so. One of the best proofs SSRI deaths are deliberately removed from trials came from a 2005 meta-analysis conducted by independent researchers of the published trials. It included 87,650 patients and all ages and found 2.28 times the suicide attempts on drug than on placebo and that many suicide attempts were missing from the trials (e.g., some of the investigators who were queried responded that there were suicide attempts they had not reported in their trials, while others shared that they didn’t even look for them). Note: SSRI suicides are almost always attributed to “pre-existing” depression, which is then used to argue that those suicides actually meant that more SSRIs rather than fewer SSRIs should be given out. Yet, in a detailed review on the subject of depression and suicide, only 26% of those who commit suicide had been diagnosed with depression before the suicide. This is analogous to many COVID vaccine injuries being blamed on catching the virus itself (e.g., many injuries are attributed to long COVID). Sadly, one of the most common causes of vaccine death is the individual developing a fatal case of COVID-19 (this has been shown within the VAERS data and I personally know of many cases where this happened). Likewise, I know of multiple cases where an individual had an asymptomatic or minor infection at the time of vaccination that then rapidly became severe or fatal. Sadly, rather than consider the vaccine’s culpability, these cases are used to argue the individual needed to have been vaccinated earlier, much in the same way SSRI suicides are attributed to insufficient “treatment” of those patients. |
|
When the side effects were reported, much like the previously mentioned “non-compliance” those effects (with the FDA’s consent) were reclassified to innocuous and misleading terms (which were often only learned after lawsuits forced the disclosure of those trials). For example: • Suicides were typically coded as “overdoses.” • Suicidal ideation or attempted suicide was coded as “depression” or “emotional lability.” • Akathisia (the violent restlessness where one feels as though they want to jump out of their skin and which typically proceeds murder or suicide) was coded as “nervousness,” “agitation” or “agitated depression.” • Abnormal thoughts (one of the most common SSRI side effects) was coded as “abnormal dreams.” • Other attempted (and frequently completed) suicides that were preceded by hallucinations were simply coded as “miscellaneous effects” (not unlike what happened with Gardasil’s most concerning injuries). Remarkably, as shown within Lilly’s own memos, even their own researchers (in Germany) were uncomfortable doing this and only did so because they Lilly’s management ordered them to. Note: Many of the trial participants testified that they suffered a severe injury from the COVID-19 vaccines which did not make it into the final report despite their best attempts to do so (e.g., providing the medical documentation showing that they did indeed have the condition or petitioning the FDA for it to be acknowledged). Maddie De Garay for example is permanently disabled (she can no longer walk alongside a variety of other debilitating symptoms) and her reaction was coded as “functional abdominal pain,” Olivia developed a malignant and unusual cancer which was coded as “moderate lymphadenopathy” (swollen lymph nodes), and Augusto Roulex almost died from a pericardial effusion, which was coded by the lead authors of Pfizer’s NEJM trial as COVID-19 (despite Augusto testing negative for COVID-19). |
|
The SSRI trials observed those receiving the drug for a relatively short period, making it impossible for many of the later onset side effects to be detected, (particularly the devastating SSRI withdrawals). This is similar to how after receiving an EUA, Pfizer and Moderna abruptly ended their placebo groups under the argument “it was unethical to withhold the life saving vaccination,” which in turn made there no longer be a control group which could prove the litany of chronic side effects following vaccination were indeed due to the vaccine. Sadly, this absence of evidence is often treated by the courts as there being “no evidence” those harms exist. Note: As you might have guessed, the patients in those placebo groups were monitored for a much longer period than the SSRI recipients, which led to many more adverse events (e.g., suicide) being documented for the placebo group. For example, Pfizer produced a meta-analysis claiming Zoloft reduced the risk of suicide by 48%, but once an additional 29 days (of recorded data) was taken into account, their SSRI instead increased the risk of suicide by 47%. |
|
Many of the trials which yielded concerning data (even with every possible attempt being made to spin them in a positive direction) were simply never published (and in many cases not disclosed to regulators). For example, in 2004, a researcher used a comprehensive summary of internal reports of GSK’s trials (made available on the internet as a result of litigation) and found that Paxil increased suicidal tendencies by 177% (likewise numerous cases of self-injury, suicidal ideation and suicide attempts never made it into the public reports of GSK’s trials). In one of the most memorable examples, after Pfizer got an antidepressant (Reboxetine) approved in Europe (but not the USA), a German institute asked Pfizer for all of their studies on it — which Pfizer repeatedly refused to do until the institute said Reboxetine would not be eligible for insurance reimbursement unless the institute had the data to see if it worked. Pfizer immediately complied, and the institute in turn concluded the drug was unsafe and ineffective. Sadly Europe’s FDA doubled down on their approval and simply unjustly attacked the institute for its conclusion. |
Putting Lipstick on a Pig
In short, much of the clinical trial industry has evolved into finding elaborate ways to put “lipstick on a pig,” which in my opinion is largely a result of the mass media, medical academics, the medical journals, and the drug regulators being unwilling to call this behavior out and demand the trials be conducted in an accurate manner that will actually predict how the products will perform once they enter the market.
Note: In a recent article, I attempted to illustrate the systemic web of corruption which led to this.
One of the saddest things about this fraud is that doctors are trained to believe all drug side effects (especially from those their specialty regularly prescribes) are “anecdotal” unless there is scientific proof those side effects are real. Yet simultaneously, relatively few of them realize that the “peer-reviewed” articles they rely upon for that proof always censors pharmaceutical side effects.
This in turn gives rise to the sad phenomenon of medical gaslighting (which for example we saw throughout the COVID-19 vaccine program).
Note: One of the best books I have found about psychiatry’s gaslighting is the aptly named Deadly Psychiatry and Organized Denial. That book was one of the primary sources for this series.
According to it, some of the most common forms of psychiatric gaslighting include the suicides “just being [inconsequential] anecdotes,” the trials not showing a statistically significant increase in suicide (rather they only showed an increase of suicidal behavior), and that SSRIs protect against suicide because they treat the undiagnosed depression that frequently causes suicide.
Sadly, this is not that different from the logic vaccine fanatics use to justify more and more boosters despite the fact they are the primary ones still getting COVID.
Conclusion
In this article, I have tried to provide the irrefutable evidence that SSRIs are quite dangerous. In my eyes, this is particularly tragic because the trials showed they aren’t effective for the majority of the recipients either, which means many people ruined their lives with drugs that offered no benefit to them in the first place.
This is particularly tragic since many effective approaches have been developed over the years for treating depression (discussed in detail here), but as there’s no money in those treatments, the SSRIs were what monopolized the marketplace.
Given how bad the clinical trial data was, it immediately should raise the question, how could these medications have possibly gotten onto the market? In the next part of the series, we will discuss the bribery which took place across the world to make that possible and examine just how far the FDA will go to protect a bad drug it is invested in regardless of how many complaints it receives from the public.
Lastly, if you are considering stopping an antidepressant, be aware very bad things can happen if you abruptly withdraw it (e.g. violent psychosis [as discussed here] or significant neurological decompensation [discussed here]). If you plan to stop an SSRI, it is strongly recommended you work with a mental health professional who has experience in this area.
For those who do not have access to one, I provided a comprehensive summary of how to safely withdraw from SSRIs and tricks to make the process a bit easier here.
A Note From Dr. Mercola About the Author
A Midwestern Doctor (AMD) is a board-certified physician in the Midwest and a longtime reader of Mercola.com. I appreciate his exceptional insight on a wide range of topics and I’m grateful to share them. I also respect his desire to remain anonymous as he is still on the front lines treating patients. To find more of AMD’s work, be sure to check out The Forgotten Side of Medicine on Substack.
Source: Original Article
Publish Date: 2024-01-11 07:35:13